Social Impact of Hair Loss
Although there are those who accept hair loss gracefully, to many, it causes significant social and psychological stress. Concerns over hair loss have been documented throughout history.
Recently, a 5000-year old body from the Neolithic Age was found frozen outside of Austria. The frozen body had a neatly trimmed beard and closely cropped hair- so obviously the appearance of hair was important as far back as 5000 years ago. One of the oldest known medical texts is an ancient Egyptian papyrus scroll. Among its remedies is an ointment for restoring hair loss consisting of equal parts crocodile and hippopotamus fat.
The ancient Greek physician Hippocrates’ interest in hair loss was stimulated by his own baldness- and indeed the name for the permanent fringe of hair that encircles the back and sides of the head has sometimes been referred to as the “Hippocratic Wreath”. We are all familiar with the story of Samson and Delilah, perhaps the most famous “hair equals virility” story of all time. During the time of Louis the XV wigs became fashionable and a number of the signers of the Declaration of Independence wore wigs when they wrote their names. In movies villains are often depicted as bald while heroes have a full head of hair.



Hair Loss Facts & Proven Solutions
In modern times over 80% of men and 35% of women will suffer from some degree of hair loss. Over 2 Billion dollars a year are spent on various treatments for hair loss. No other facial feature changes one’s appearance as much as the presence of a normal hairline. It is only recently that the shaved head has become an acceptable look and most likely it is a trend that will come and go like other fashion statements.
The bad news is that there are a number of scam treatments that prey on people who are desperate, gullible and willing to try anything to retain their hair. The good news is that a number of clinically proven medical and surgical techniques that work have been developed over the years that work. Among these are Rogaine, Propecia, and well performed Follicular Unit Transplantation.
Dermatologists and other physicians are often asked to evaluate patients for hair loss. Apart from establishing the etiology of hair loss, patients want to know how the hair can be restored. Hair transplantation has become a significant treatment tool in the armamentarium for hair loss. A survey by the International Society of Hair Restoration (ISHRS), estimated that over 80,000 hair transplant procedures are performed yearly in the United States alone. It is ranked as the second highest cosmetic procedures done on men.

Causes of Hair Loss
Historically, Male Pattern Baldness (MPB) is the most common indication for hair transplantation. It is caused by exposure of hair to the androgen Di-Hydro-Testosterone (DHT) which is a metabolite of testosterone created when testosterone reacts with the enzyme 5-alpha- reductase. When susceptible scalp hairs are exposed to DHT they become finer and shorter with each recurring growth cycle eventually leading to baldness.
Di-Hydro Testosterone (DHT)
The severity of MPB varies dramatically and can be as mild as minor recession of the hairline or as severe as complete loss of the hair on the superior aspect of the scalp. Genetically determined differences in the sensitivity to DHT explain these variations between people. However even in the most severe case of MPB, hair loss does not occur in the horseshoe shaped ring of hair in the occipital and lateral fringe areas of the scalp. This is because this hair is not sensitive to the effects of DHT.
Types of Hair Loss
Over 80 million Americans experience hair loss in their lifetime with hereditary hair loss (androgenetic alopecia) being the most common cause of balding. An estimated 50 million men and 30 million women in the United States are affected male and female pattern baldness to some extent, respectively.
Other types of hair loss that men and women commonly experience include traction alopecia (hair loss caused by wearing very tight hairstyles) and alopecia areata (an autoimmune disease that causes the hair to fall off in clumps).
Why Hair Transplants Work
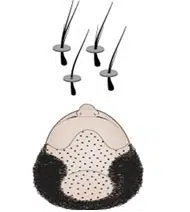
The first description of hair transplantation was actually written by Dr. Okuda in Japan in the 1930s. He used hair transplantation to treat burn victims during WWII. However records of his work were lost after the war. In 1950 Norman Orientreich MD rediscovered the process and successfully performed the first hair for transplant in the United States for patients with MPB.He proved when “donor” hair from the permanent horseshoe shaped fringe area on the back and sides of the head was moved to the balding “recipient” area on the top of the scalp that it continued to grow and did not fall out. Donor hair from the fringe area retains its genetic programming even after it is moved and stays insensitive to DHT. It is this property of donor hair remaining insensitive to DHT and not being affected by local properties in the recipient area that enables transplanted hair to grow. Orientreich called this property “donor dominance” and it is the property that makes hair transplantation possible.
It is important to point out that this fringe of donor hair is a finite and limited area that can only produce a finite and limited amount of donor hair. The concept of a limited donor supply is an important concept in hair transplantation as it places a limit on what we can accomplish.
Although Orientreich demonstrated that we could move hair and it would indeed grow, the original procedure often created an unnatural look and therefore had limited application. The desire to improve naturalness has led to many improvements in the technique, more natural results and a broader range of applications.
History Hair Transplantation


Standard Punch Grafting (Original “Old’ Technique)
I want to state from the outset that this technique is old and outdated and only being discussed from a historical perspective to better understand how more modern techniques evolved. From 1950 to the early 1980s the only procedure available to the public was the technique made popular by Orientreich called Standard Punch Grafting. This procedure used large circular grafts (often called “plugs”) harvested by round punches. Each graft was about the size of a pencil eraser and contained as much as 20 to 30 hairs per graft. Only 50-100 of these grafts were used at a time. These large grafts had to be spaced rather far apart due to the constraints of blood supply and this led to the “dolls head” look commonly associated with transplants of the past. In addition this technique wreaked havoc on the donor area. The punches used to harvest these “plugs” from the donor area often left a scarred checkerboard pattern in the back of the head.
The only way to resolve this dolls head appearance was to do multiple procedures in an attempt to fill in the gaps between the plugs. Many patients frustrated and disappointed with the initial results simply did not finish the process. Even if patients did finish the process other problems with naturalness occurred over time due to the inefficient use of the limited donor supply. To fill in the gaps, physicians were forced to use up the entire donor supply in a very small area. Very unnatural islands of grafted hair became noticeable over time as hair loss progressed and receded away from these heavily grafted areas.
To make matters worse there was now no donor hair left to fix the situation. It was during this time that physicians learned to appreciate and take into account the progressive nature of hair loss when planning hair transplantation in patients with MPB. . As stated above the technique of Standard Punch Grafting is obsolete and no longer used. Unfortunately many patients with this old technique are still walking around and people mistakenly think that they represent hair transplants today.
Combination Mini-Micro Grafting
The desire to improve naturalness led to the use of smaller grafts. By the late 80’s and early 90’s a technique called Mini-Micro grafting became the standard. Graft size had been reduced to 4-12 hairs per graft. Small slit incisions were now used for the recipient area instead of round punches. The decreased vascular trauma associated with these smaller slit incisions enabled a larger number of grafts to be placed closer together in a single session. Procedure size increased to an average of 400 to 800 grafts per session.
Donor harvesting and graft preparation techniques improved also. Donor tissue was no longer harvested with individual round punches but rather from a single strip of donor tissue (a process called strip harvesting). The harvested strip was subsequently divided into individual grafts. This produced less scarring leaving behind a single linear scar rather than a checkerboard pattern. Strip harvesting also increased the total amount of hair that could be harvested from the donor area. Mini-Micro grafting was a vast improvement over Standard Punch grafting but the results were still not totally natural under all conditions and room for improvement still existed.
Follicular Unit Transplantation
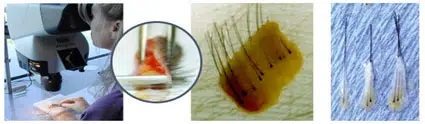
By the mid 90’s, Follicular Unit Transplantation (FUT) became the state of the art procedure used in hair transplantation. This revolutionary advance occurred when physicians observed that hair grows and exits the scalp in tiny, naturally occurring groupings of 1-4 hairs called follicular units.
With this observation physicians began using microscopic magnification to create grafts that keep these natural groupings intact. These 1-4 hair grafts, called Follicular Unit (FU) grafts are so tiny they can be placed in micro-incision about the size of a needle. The reduction in graft and recipient site size allowed for larger numbers of grafts to be placed closer together with less danger of vascular trauma. By the late 90’s procedures consisting exclusively of FU grafts could range from 1500-2500 depending on the size of the area being treated. FU grafts can be placed at densities of about 20-30 grafts/cm which is significantly closer than with mini grafts.
These tiny grafts replaced hair with the same size groupings found in nature.
As time progresses further advances continue to be made in the way follicular unit transplantation is performed. Some the more current advances include:
- Larger sessions in properly selected patients.
- Placing the grafts at higher densities in properly selected patients.
- The option of using coronal or lateral incisions in the right situation
- Better donor closure techniques that leave less donor scarring such as the trichophytic closure
- Better holding solutions to improve survival
- A better understanding of the principles of naturalness and density



The Development of Follicular Unit Extraction (FUE)
Over the last few years a very important new innovation in the way hair can be harvested has developed. For more information about follicular unit extraction (FUE), go to FUE OVERVIEW. This is really not a new technique as much as it is a new way to harvest the donor grafts.
However, it has had a significant impact on the field. It has rapidly become the most popular procedure formed. In 2005 ~95% of all HT procedures performed were FUT with only ~5% being FUE. Today in 2018 ~55% of all procedures performed are FUE and virtually every physician that did FUT has now added FUE to some extent.
There is also a growing number of physicians that do FUE only. This is a controversial subject because although the FUE procedure is an excellent procedure for many patients, there are still a significant number who would benefit more from FUE plus FUT as a combination. For those who cannot do the FUT, they will have some limitations in what they can offer.