


Hairline
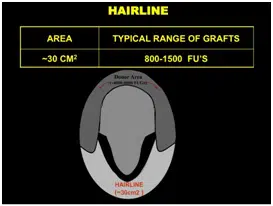
Hairline Patients often come in early when they are just early receding hairline. The area of the hairline can range from 10 cm2 to 30 cm2 if there is only a little temporal recession or if the weakness extends along the hairline. It will also change if we are bringing the hairline down and doing temporal points.
Typically, we recommend between 800 to 1500 grafts for a hairline. If we are doing Temporal points, it may add another 150 grafts per side.
Front Third
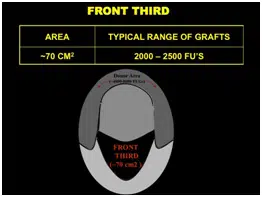
The Front third includes the hairline and the central core. It is approximately 70 cm2. It contains the frontal tuft, which is a very important area for creating the illusion of density.
Typically, we recommend between 2000-2500 grafts for the front third.
Front Half
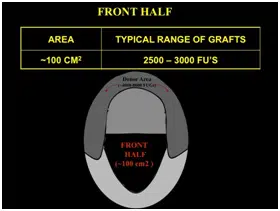
The Front Half is approximately 100 cm in size.
Typically, we recommend between 2500 to 3000 grafts when doing the front half.
Front Two Thirds
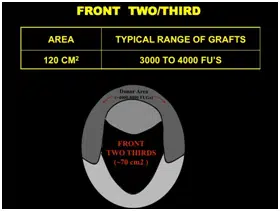
The Front Two Thirds is approximately 120 cm2 in size.
Typically, we recommend between 3000 to 4000 grafts when doing the front two thirds.
Crown
The Crown can range from 60 to 100 cm2. We typically do not want to place too many grafts in the crown until we are certain a patient has enough grafts to make sure his front two thirds will reach his expectation. However, in the average patient, it is usually safe to do at least 800-1200 grafts in the crown with the goal of turning a shiny bald spot into an area that just looks like it is thinning. But more than this number should not be done until we are sure a patient has enough grafts for the front.
We usually recommend between 800 -1500 grafts for the crown.