Mens Hair Loss
Male androgenetic alopecia or male pattern baldness (MPB) is the most common cause of hair loss in men and a common indication for hair transplantation. To have a successful hair transplant, we need to meet the patient’s goals of both naturalness and density.
Creating naturalness is achieved by using 1-4 hair FU grafts to mimic patterns and distributions of hair found in nature. Creating a natural hairline is most important. A hairline should initially appear irregular, soft, and ill-defined but gradually take on more definition and substance as it moves posteriorly. Creating too abrupt or straight of a hairline does not look natural and is a common mistake made by beginning transplant surgeons.





Selective Graft Distribution
To accomplish this goal only 1 hair FU grafts are in the anterior portion of the hairline with a shift towards 2 hair FU grafts as we move toward its posterior portion. Behind the hairline, density is more important and a shift toward larger 3-4 hair FU grafts is made. This is called selective distribution of grafts and is an important technique used in hair transplantation. It is also important to make incisions at the angle and direction that follows the natural flow of hair.
The amount of density that we can ultimately create will depend on the severity of hair loss and the supply of donor hair. The severity of MPB varies dramatically and can be as mild as minor hairline recession of the hairline or as severe as complete loss of the hair on the superior aspect of the scalp.
Hair Loss is progressive at an unpredictable rate. It is very hard to predict how severe a pattern will develop in a patient when they are young. Family history helps a little but is not very reliable. Probably the best predictor is the age and severity at which hair loss begins.
A patient that develops significant hair loss at a very early age will most likely end up with severe hair loss, while a patient that only begins to recede in his 40’s or 50’s will most likely have a less severe pattern.
Planning Coverage and Density
Predicting and communicating the degree of density and the area of coverage that we can provide a patient is one of the most difficult skills to learn in hair transplantation. Since most patients have enough donors to cover the front half of their head we usually suggest that patients treat the front half first. When they are satisfied with the front we can move to the crown if there is a donor left.
The general dogma is to plan for the worst case scenario and maximum hair loss. We can be more aggressive if a patient is older with minimal hair loss. The most difficult patient to treat and the ones who need to be educated the most about realistic expectations are:
- Patients that want their hairline too low
- Patients that are just beginning to thin and don’t want to “see scalp”
- Patients with severe hair loss in both the front and crown who want full coverage everywhere
- Young patients with early hair loss in whom we can’t be sure how severely they will progress
Womens Hair Loss
Female androgenetic alopecia or female pattern baldness (FPB) is the most common cause of hair loss in women. The pattern of hair loss in FPA is different from MPA in that the hairline is usually not affected but there is diffuse thinning in the central scalp behind the hairline.
Ludwig and Olsen described the pattern slightly differently. Ludwig described FPA as occurring in a caudal and centrifugal pattern in which hair in the hairline is maintained, though it may thin to varying degrees.




Female Hair Loss Patterns
Ludwig created a scale in which she divides FPA into Ludwig Type 1, Type 2 and Type 3 with severity getting progressively worse as we move from 1 to 3. Olsen described a “Christmas tree” pattern of loss which begins as a “widened part” but evolves into a zone of hair loss that is widest anteriorly at the hairline and gradually narrows, with ragged borders, more posteriorly.
Females have some special issues that need to be addressed before deciding if they are a good candidate for surgery. First of all, females are prone to other etiologies of hair loss. If there are any signs and/or symptoms suggestive of an endocrine, metabolic or dermatological cause, they should be investigated and treated appropriately. It is also important to rule out temporary hair loss caused by severe emotional or physical stress leading to telogen effluvium. However, the majority of females seeking transplantation for hair loss have no apparent cause other FPB.
Female Shock Loss & Hairline Solutions
Females are much more susceptible to the postoperative complication of “shock loss” or “telogen effluvium” of existing native hair still present in the recipient area. Postoperative shock loss occurs when pre-existing native hair is triggered to go into a telogen (resting) phase by the local stressors of surgery.
In men, this can occur from 10% to 20% of the time while in females it occurs more frequently, almost 30% to 50% of the time. In general, this shock loss is temporary, occurring about 2-3 months after surgery and resolving in about 4-6 months. However, in some situations, it does not totally resolve, leading to a less dense result. Women need to be warned about this before surgery.
Another abnormality quite commonly found in females is genetically high hairlines that give the appearance of a large forehead. This may be the result of heredity or secondary to a brow lift. Women with this situation feel uncomfortable wearing their hair up or back and often wear bangs.
Hair transplants are an excellent tool with which to lower the hairline. An alternative method of lowering the hairline is with the hairline advancement flap discussed earlier in this.
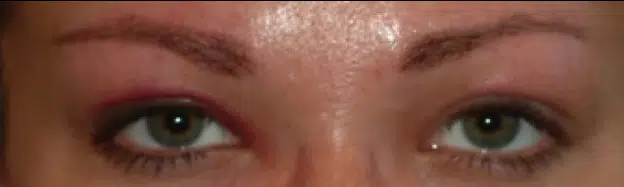
Eyebrows
Eyebrows play an essential role in facial aesthetics. But just like the hair in your head, your eyebrow hair can thin or stop growing. Many women and some men seek help for thinning or absent eyebrows. With the refinement in follicular unit transplantation, eyebrow loss can be slowed and normal appearing eyebrows can often be restored.
Loss of eyebrow hair may be due to trauma such as burns and avulsions; medical conditions such as hypothyroidism; or genetics. It may also be self-inflicted due to long-term eyebrow plucking, or trichotillomania, which is an obsessive-compulsive hair pulling disorder.

How Eyebrow Transplants Work
Approximately one-third of patients attribute their thin eyebrows to inheritance and are born with them. It is important to treat and stabilize any underlying condition before transplantation. Enough time needs to pass after treatment to allow any potential re-growth of native hair to occur. Prior permanent make-up or tattooing is not a contraindication to eyebrow transplantation as the hairs will cover the tattoo.
If the tattoo is to be removed it should be done so before transplantation. If the eyebrow tattoo was placed in an unaesthetic location, which extends outside the normal boundaries of the eyebrow, it can be surgically removed leaving a fine line that can then be easily concealed with the transplanted hair.
It is important to understand the normal shape and patterns of eyebrows in order to recreate these shapes. The eyebrow can be divided into three parts; the medial portion is the head; the central portion is the body; and the lateral portion is the tail. An arch occurs along the eyebrow in women. The direction and density of hair is different in each of these parts. The hair is less dense and directed upward in the medial head. The hair is most dense and is directed more horizontally in the central body.
However, in the body, the cephalic-most hairs tend to grow at a slightly caudal angle, while the caudal-most hairs tend to grow at a slightly cephalic angle, resulting in a cross-hatching effect and a greater illusion of density. In the tail, hairs are less dense once again and directed horizontally. Only 1 and 2 hair grafts are used in the eyebrow with the 2 hair grafts designated for the thicker body of the eyebrow.
Typically 200-250 grafts are transplanted into each eyebrow. These hairs are harvested from the occipital donor area as with any FUT procedure. The recipient incisions have to be angled very acutely to ensure the hairs lay flat against the skin and don’t stick out. Patients have to be told that the hair will grow long like normal scalp hair and that they will need to trim the hair to the desired length on a regular basis.
If after surgery, the shape of the eyebrow is not exactly what the patient wanted it can be sculpted afterward with electrolysis. Most patients get excellent results and are extremely grateful.
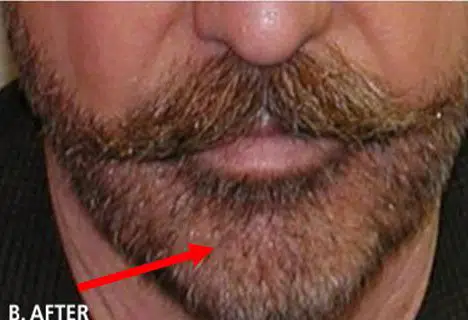
Beard & Moustache
Many men have bald spots or weak patches of hair in their beard or mustache. Follicular unit transplantation is ideal for filling in these areas. Normal facial hair usually consists of very thick and coarse 1-hair units. It is hard to find this degree of coarseness in the occipital donor area. Therefore, 2-hair grafts are usually used instead of 1-hair grafts in an attempt to match the thinness of the coarse beard hair. Some men simply want a thicker beard.



Scar Repair
Hair transplantation can be used as a scar treatment to treat areas of scarring on the scalp caused by different types of physical trauma. These could include scars caused by burns, explosions, accidents. Sometimes the scarring is iatrogenic and produced by surgical procedures such as face lifts, brow lifts, radiation treatment; or removal of a scalp tumor such as a hemangioma. Special considerations are needed when transplanting into areas of scarring.



Hair Grafts and Scar Challenges
The issue of adequacy of the blood supply to the scar tissue often arises. In addition to leading to poor graft survival, this limited blood supply can potentially leave the recipient area more vulnerable to infection, further ischemia and necrosis. Although these are legitimate concerns, experience has shown that the blood supply in scar tissue is often sufficient to accommodate the appropriate placement of FU grafts.
In general, one should always perform the first transplant with a smaller number of grafts placed further apart so as not to stress the blood supply. It is also prudent to wait longer in between sessions. With scar tissue, it is better to plan on doing multiple, smaller sessions that succeed rather than one large session that fails greater oxygenation to the tissue.
Not all scars are the same and scar thickness can have an effect on transplantation. Some scar tissue is thick and tough, while other scar tissue is thin and friable. With thick hypertrophic scars, there is concern that the incisions will not gain access to the blood supply. In these situations, one should err on the side of making the incisions slightly deeper.
Transplanting into thin atrophic scar tissue, such as that created by post-radiation injury, creates a different, and in our opinion, a more difficult problem. The recipient area in this thin, poorly vascularized tissue is more prone to ischemia. In addition, the shallow skin makes it difficult to create incisions deep enough to house even tiny FU grafts.
Making the incisions at a more acute angle can increase the length of the incisions, and create a posterior “pocket” to house the graft. Carefully using a small amount of tumescent solution (without epinephrine) can temporarily distend the skin, making it easier to create these more acutely angled incisions.
On several occasions, we have noticed that after the first conservative transplant into an area of atrophic (thin tissue) scar it becomes thicker. It may be that the FU grafts act like multiple tiny skin grafts, and also may stimulate angiogenesis.
Hairline Repair
Before Follicular Unit transplantation, there were many people who had transplants who were unhappy with the results. They had hairlines that looked very unnatural.
With FUT, these can often be corrected by either punching out the old graft, redistributing, and adding newer finer grafts to camouflage the old grafts or a combination of both.